What Is MRI Acceptance Testing and Why Does the MHRA Recommend It?
- UKMR

- 3 hours ago
- 11 min read
Introduction
Installing a new MRI scanner is a significant investment — financially, clinically, and operationally. But once the engineers pack up and leave, how do you actually know the system is performing as it should? That's exactly the question MRI acceptance testing is designed to answer.
In the UK, the Medicines and Healthcare products Regulatory Agency (MHRA) strongly advises that independent acceptance testing is carried out on all newly installed MRI systems before they enter clinical use. This post explains what acceptance testing involves, why independence matters, what the report looks like, and what you risk by leaving it out.

What Is MRI Acceptance Testing?
Acceptance testing is a structured evaluation carried out after an MRI scanner has been installed and before it starts scanning patients. It confirms that the system is safe, that it meets the manufacturer's published performance specifications, and that it is ready to serve as the baseline for all future quality assurance.
A thorough acceptance test covers several key areas:
Imaging performance: Signal-to-noise ratio, image uniformity, geometric distortion, slice thickness accuracy, and ghosting artefacts
RF and gradient system performance: Including EPI stability and spectroscopy tests where relevant
Coil evaluation: Testing each RF coil supplied with the system to confirm it performs within specification
Magnetic field mapping: Confirming the location of the 0.5 mT isocontour — the boundary of the MR Environment — matches what was planned at the design stage. The 0.5 mT line defines the extent of the MR Environment and is the critical reference for controlled access zone design and passive shielding requirements
Site safety review: Checking that zones, signage, access controls, and emergency procedures are correctly in place before staff and patients enter the environment
Crucially, independent acceptance testing goes beyond simply repeating the manufacturer's commissioning tests. We design our test programme to push the scanner under demanding, real-world conditions — for example, a 10-minute continuous EPI acquisition to stress the gradient system and verify thermal stability under sustained load. These extended tests can reveal performance limitations that would never surface under the shorter, controlled conditions of standard commissioning, and that only become apparent when the system is driven hard in clinical use.
This last element, the site safety review, is often underestimated. It's not simply a walk around the room with a checklist. An HCPC Clinical Scientist will assess whether the MR Controlled Access area is appropriately designed, whether the MR Environment boundary (>0.5 mT) is correctly established, including verification that any passive shielding installed to reduce the magnetic field to safe levels in areas accessible to the general public is performing as intended, whether emergency quench procedures are documented and understood by staff, whether signage meets MHRA and IPEM requirements, and whether any risks have been introduced by the building environment itself — for example, nearby metalwork, lift shafts, or electrical plant that could create interference.
Why Does the MHRA Recommend Independent Testing?
The MHRA's Safety Guidelines for Magnetic Resonance Imaging Equipment in Clinical Use are unambiguous on this point. Section 5.3.2 states:
"Project teams are strongly advised to arrange for independent acceptance testing of the MR scanner by an MR physicist. The benefits of this are that: it provides an independent assessment of performance; it provides a baseline for further regular quality assurance; it identifies any corrective action required before clinical use commences. The acceptance process may also include independent electrical safety testing, independent confirmation of the 0.5 mT (5 Gauss) line, and independent confirmation of noise levels." — MHRA Safety Guidelines for Magnetic Resonance Imaging Equipment in Clinical Use, Section 5.3
The key word is independent — meaning carried out by an HCPC Clinical Scientist who is not employed by, or in any way affiliated with, the scanner manufacturer.
There are good reasons for this. Manufacturers conduct their own commissioning tests, but these are performed against their own specifications, by their own engineers, using their own protocols. An independent Clinical Scientist brings no conflict of interest. Their role is to verify what the manufacturer claims — and to identify any gap between specification and reality before patients are exposed.
Independent testing also establishes a verified, third-party baseline. Every future quality assurance measurement taken on that scanner will be compared against this starting point. If that baseline is inaccurate or incomplete, your entire QA programme is built on unreliable foundations.
What Can Go Wrong — And What Can Be Caught
CASE STUDY |
During acceptance testing of a newly installed clinical MRI system, physicist identified failures in both the RF noise tests and SNR measurements — the scanner failed against published specification.
Investigation traced the fault to work carried out on the penetration panel after the RF shielding contractor had completed and signed off their tests. A single washer had been omitted from one of the penetration fittings, leaving a small but significant gap in the RF shield. The result was RF interference entering the magnet room, producing image artefacts.
The fault was identified and rectified on the same day. The fitting was correctly reassembled, shield integrity restored, and all acceptance tests repeated and passed. The scanner entered clinical service with a verified performance baseline — a fault that would have caused problems in clinical imaging after commissioning. |
This case illustrates precisely why independent acceptance testing matters. The artefacts produced by this fault were intermittent and subtle — the kind easily dismissed as patient movement or minor equipment noise in day-to-day use. Without independent testing, there would have been no reason to look for a shielding defect, and no baseline against which any degradation would register.
Had the scanner gone live untested, it would have operated with a compromised RF shield from day one. The fault would likely have remained undetected indefinitely — with no baseline to reveal that anything was wrong.
What Does the Report Look Like?
Following acceptance testing, you should receive a formal written report from your physicist. This is a document you will refer to throughout the lifetime of the scanner, so it matters what it contains.
A comprehensive acceptance testing report will typically include:
System Performance Tests: We begin by repeating the manufacturer's own commissioning tests to confirm the scanner is within the manufacturer's specification before proceeding to independent testing. Measured values are compared against both manufacturer specifications and recognised reference standards, providing a complete, verified performance picture.
Multi-channel coil QA: Each coil element SNR is measured individually and recorded. This is particularly important for longitudinal monitoring — at annual QA, these per-element values can be directly compared against the acceptance baseline. Notably, not all coil elements carry manufacturer SNR tolerances, meaning they fall outside the pass/fail criteria of standard manufacturer testing. Independent testing captures these elements regardless, providing a more complete reference record.
Magnetic field survey data: Including the measured location of the 0.5 mT isocontour confirmed on your actual site.
Full Safety Audit against MHRA guidelines: A comprehensive on-site audit of the premises against current MHRA requirements — covering controlled access zone design, signage, access controls, and the physical MR environment. Note this covers the physical site and does not include document review.
A clear pass/fail summary: Identifying any parameters that fall outside specification and the recommended corrective action.
Recommendations for your ongoing QA programme: Tailored to your specific scanner model and clinical activities — including manufacturer-specific QA protocols, best practice for specialist programmes such as the National Breast Screening Programme, and requirements for specialist activities such as spectroscopy and fMRI.
This report forms part of your site's governance documentation. For CQC-registered providers, it is evidence that your scanner was properly validated before entering clinical use. For research sites, it is often a requirement of ethics committee approval and trial protocols. For any provider, it is the document you reach for when a scanner's performance is questioned — whether by a regulator, an insurer, or a clinical team.
What Happens If You Don't Do It?
The consequences of skipping independent acceptance testing range from inconvenient to serious:
Undetected performance issues. A scanner that passes manufacturer testing may still underperform in your specific environment. Environmental factors won't surface without independent measurement in situ.
A flawed QA baseline. Without an independently verified starting point, you have no reliable way to detect when performance degrades over time. Drift goes unnoticed; problems accumulate.
Regulatory and governance exposure. For CQC-registered providers, Regulation 12 of the Health and Social Care Act sets a clear expectation:
"Providers must ensure the safety of their premises and the equipment within it. They should have systems and processes that assure compliance with statutory requirements, national guidance and safety alerts." — CQC, Regulation 12: Safe Care and Treatment
Independent acceptance testing — with a formal written report — is precisely the kind of documented system and process that satisfies this obligation. The absence of such a report, particularly where MHRA guidance has not been followed, can constitute a governance failure and become an inspection finding. For research sites, the absence of an accepted baseline may also invalidate imaging data.
Clinical risk. In diagnostic imaging, image quality directly affects diagnostic confidence. Subtle artefacts or resolution issues that are present from day one may go unnoticed — until they contribute to a missed finding or a repeated scan.
Specialist Systems: MRI in Radiotherapy
For centres using MR Radiotherapy systems, acceptance testing requirements go beyond those for a standard diagnostic installation. Geometric accuracy is paramount: where a diagnostic image can tolerate minor distortion without clinical consequence, an RT planning image that is geometrically inaccurate can directly affect treatment margins and target delineation.
Siemens Healthineers' Commissioning and Quality Assurance (QA) for MAGNETOM Systems in Radiation Therapy sets out the expectation clearly:
"This guide considers various methods for QA addressing the variants of the system which may influence geometric accuracy and other factors for MRI... To evaluate the performance of an RF coil during commissioning, its signal-to-noise ratio (SNR) can be measured. Several SNR measurements can be recorded, and these should serve as baseline measurements for calculating standard deviation. This standard deviation can subsequently be employed as a benchmark during the regular System QA to ensure that the coil is performing optimally." — Siemens Healthineers, Commissioning and Quality Assurance (QA) for MAGNETOM Systems in Radiation Therapy
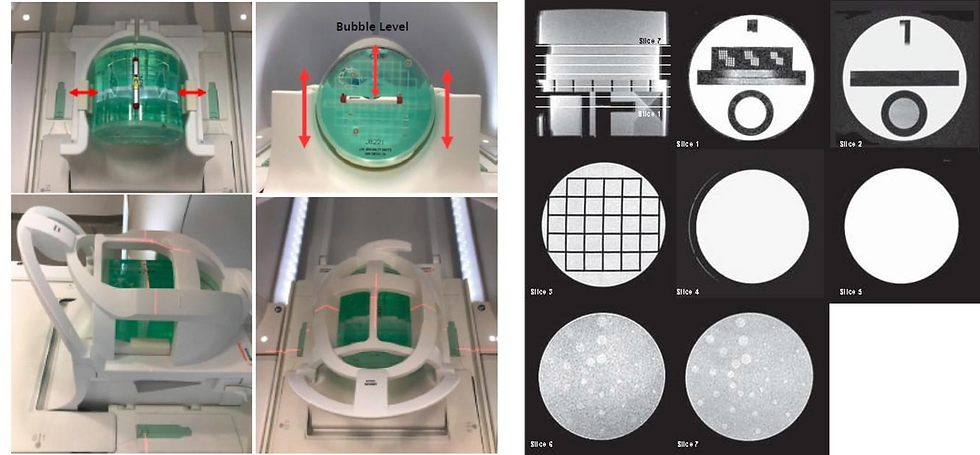 |
ACR Large Phantom positioned within the MRI scanner Head Coil and representative images used to assess slice positioning, slice thickness accuracy, geometric accuracy, image uniformity, ghosting, and low-contrast object detectability during acceptance testing. |
For MR Radiotherapy installations, the acceptance testing programme will typically include dedicated ACR Phantom QA testing to evaluate image quality parameters including low contrast detectability, high contrast spatial resolution, and slice thickness and position accuracy. It will also include geometric distortion assessment across a large field of view — a requirement specific to RT use, where geometric accuracy within 2 mm (or 1 mm for certain applications) is required across the full imaging volume — as well as laser isocenter verification and table accuracy and reproducibility testing.
Establishments deploying MR Radiotherapy systems should ensure their acceptance testing physicist has specific experience with these installations, and that the testing programme is designed to meet the requirements of the clinical treatment planning workflow, not just standard diagnostic QA standards.
When Should Acceptance Testing Be Booked?
Timing matters. Acceptance testing should be arranged before the scanner goes into clinical use, but ideally the physicist should be involved earlier than that — at the point of site planning or procurement, where they can advise on the design of the magnet room, shielding requirements, access control zones, and the specification of the scanner itself.
At minimum, you should be in contact with an independent physicist before the manufacturer's engineers arrive on site. This allows the physicist to observe or review the manufacturer's commissioning process, agree the testing schedule, and ensure the independent tests can be completed before the first patient is booked.
In practice, for a standard installation at a private clinic or NHS site, independent acceptance testing typically takes one to two days on site, with the written report delivered within a few weeks. The exact timescale depends on scanner complexity, the range of coils to be tested, and the scope of any additional research or specialist protocol testing required.
Where Acceptance Testing Fits in the Project Timeline
MRI installation projects typically follow the RIBA Plan of Work stages. The table below maps the key UKMR touchpoints:
RIBA Stage | Project Activity | UKMR / MR Clinical Scientist Contribution |
0–1 Strategic Definition & Briefing | Service need identified; project brief developed | Independent advice on scanner selection, safety requirements, acceptance testing specifications, and QA requirements. |
2–3 Concept & Spatial Design | Layout options and design coordinated | Review of MRI suite layouts, zoning, magnetic field containment, RF shielding strategy, controlled areas, and penetration schedules. |
4 Technical Design | Detailed design completed | Review of vendor drawings, shielding specifications, MRI safety systems, and development of acceptance testing and commissioning plans. |
5 Manufacturing & Construction | Installation and fit-out | Technical support during installation, site inspections, and preparation for acceptance testing. Independent RF shielding verification prior to scanner installation. This is a critical project hold point. |
6 Handover & Commissioning | Scanner commissioned and handed over | Post-manufacturer commissioning: independent acceptance testing, system performance verification, multi-channel coil QA, PACS and worklist connectivity verification. Site readiness safety audit: full on-site audit against MHRA guidance before clinical use begins. |
7 Operation | Clinical service begins | Establishment of baseline QA data, optimisation support, annual QA reviews, and ongoing MRSE / MRI physics support. |
Three milestones in particular should be treated as hard hold points in the project programme: independent RF shielding verification before the magnet is installed; post-commissioning acceptance testing before the first patient is booked; and the site readiness Safety Audit confirming MHRA compliance before clinical operation commences.
Who Should Carry It Out?
The MHRA is specific: acceptance testing should be performed by an MR Physicist — ideally one who is HCPC-registered and has demonstrable, hands-on experience with MRI systems across a range of field strengths and manufacturers. This is not a task for a radiographer, or an applications specialist, however capable they may be in their own discipline. The depth of technical knowledge required — from RF physics and gradient performance to magnet field behaviour and safety zone compliance — is the product of specialist training and clinical practice.
UKMR provides independent acceptance testing services across the UK, working with NHS trusts, private providers, and research institutions. Our testing is carried out by HCPC-registered Clinical Scientists with specialist MRI physics expertise, fully independent of any scanner manufacturer.
Frequently Asked Questions
How long does MRI acceptance testing take?
For most standard clinical installations, on-site testing takes one to two days. Larger sites, multi-coil systems, or scanners intended for research use may require more time. The written report typically follows within two to three weeks.
When in the installation process should I book it?
Ideally, contact your independent physicist before the manufacturer arrives on site. At the very latest, acceptance testing must be completed before the scanner enters clinical use. Booking at short notice after installation is always possible but may limit the physicist's ability to observe the manufacturer's own commissioning process.
Does acceptance testing replace the manufacturer's commissioning?
No — the two processes are complementary. Manufacturer commissioning establishes that the scanner is operational. Independent acceptance testing verifies that it performs to specification in your specific environment, and that the site is safe and compliant.
Is acceptance testing a legal requirement?
The MHRA's guidance is advisory rather than statutory, but it represents the expected standard of practice. For CQC-registered providers, failure to follow MHRA guidance can constitute a governance failure. For research sites, it is frequently a contractual requirement of the trial sponsor or ethics committee.
What if issues are found during testing? This is exactly why testing is done before clinical use. Any parameters outside specification are documented in the report, with recommended corrective action. The manufacturer is typically responsible for addressing scanner performance issues identified at acceptance. The physicist's report gives you the independent evidence to require that they do so.
Conclusion
Acceptance testing is not a box-ticking exercise — it's the foundation on which safe, high-quality MRI practice is built. The manufacturer's commissioning process tells you the scanner works. Independent acceptance testing tells you it works in your building, for your patients, to a verified standard that your team can monitor and defend.
If you're planning a new MRI installation, it's worth addressing sooner rather than later.
Get in touch with the UKMR team to find out how we can support your next installation.
Comments